
Angelika Michael has always been playing soccer with a passion, ever since he was a little kid. Here in San Francisco, he's been in a pickup game every Tuesday for many years, and he religiously sticks to his routine, rain or shine. One Tuesday in June this year, however, he came home early from a game, cursing like a sailor. Als always, he had given his last in the game, but had tripped and fallen hard on his shoulder. Michael knew right away that his collar bone was fractured from experience, as many years ago he'd injured this delicate bone on the opposite side during Judo training. So we called our primary care physician the next day, who told us to get it x-rayed and that we should drive to the emergency room for that.
We usually try to avoid visits to the emergency room at all cost, because we know from experience that the waiting times there are unbearably long, and there's total chaos because you share the area with all the crazies, the wretched and the huddled masses of the City of San Francisco. It's quite interesting to hang out there for social studies, but if you're not doing so well yourself it gets old very quickly. Under Obamacare, patients are supposed to limit emergency room visits to real emergencies, which was supposed to reduce their workload significantly, because previously the ER was the only to-go place for people without health insurance as no regular doctor would see them.

But Obamacare actually had the opposite effect. There's a severe shortage of primary care physicians in the United States, estimates run from about 20,000 additional doctors needed until the end of 2020. Now, with the increasing number of people having access to health insurance, the situation is getting worse because those newly insured need additional doctors. It's not uncommon nowadays having to wait 4-6 weeks for a doctor's appointment, which is unacceptable if you have an urgent health problem, even if it's not life-threatening. Because of this dire situation, patients are heading in droves to the emergency rooms once again. On top of that, many states have extended their "Medicaid" social medicine program under Obamacare. It provides health benefits to people in the lowest income categories. But many doctors simply refuse to see Medicaid patients, because the rates covered by the Medicaid insurance are significantly lower than the rates paid by regular insurance companies, and low-income patients have no choice but to head to the nearest emergency room once again.
But back to Michael: Spread all across the city of San Francisco, there's a number of emergency rooms, and if a patient is still able to get there without an ambulance, they need to decide on which one to head for. A few of those ERs take appointments, that's helpful for patients who aren't already on their last legs. But if you think about it, the idea is quite absurd, as the concepts of "appointment" and "emergency" don't really fit well together. We picked an ER in the Castro district, because it's located in a relatively calm neighborhood and it's only 10-15 minutes driving distance by car from our place.
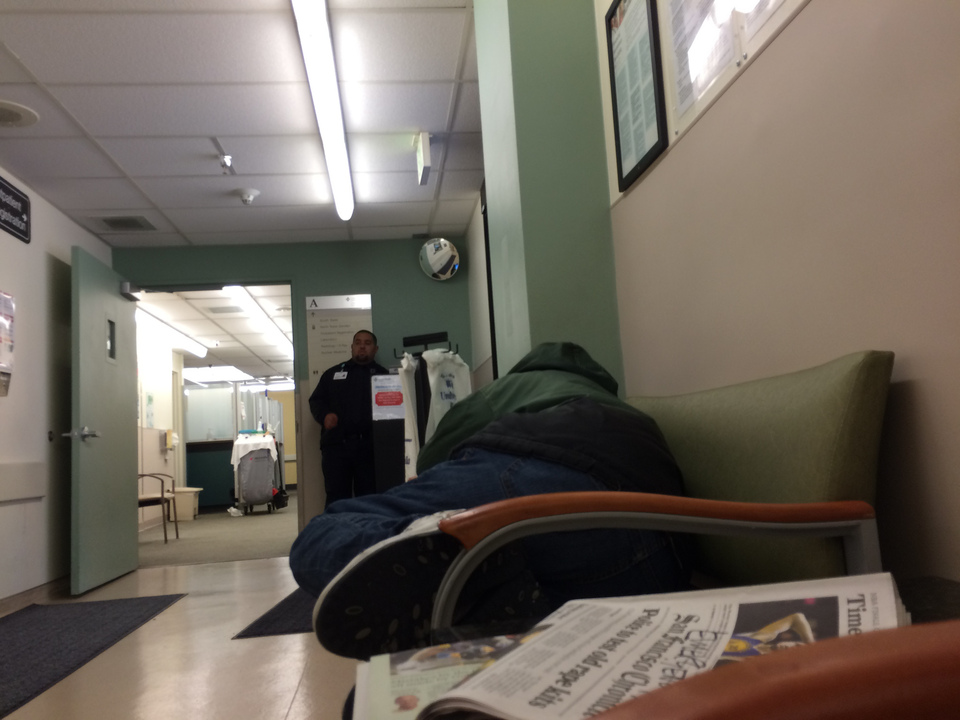
Since Michael didn't have a life-threatening condition, we had to wait more than an hour until finally someone took pity on us and made the x-ray. While we were waiting, two emergency patients were dropped off by ambulances, and a homeless person made herself comfortable on the chairs next to us in the waiting area. She had all of her possessions with her, and lied down to sleep, stretching out over three adjacent chairs. After a while, ER staff called security and it turned out that the woman needed a place to sleep in a homeless shelter. The security folks promised to make the necessary calls to help her out. Apparently, this kind of thing happens quite frequently.
Then the door flew open, in walked a loudly moaning woman, and another security guard started to worry and asked what was going on. The woman quickly started to chit-chat with him and all of a sudden completely forgot about the moaning. Four young girls visiting from the UK were all buzzing around the waiting area, all of them chipper and in apparently perfectly healthy condition. The ER doctor didn't seem to be amused. A nurse kept complaining loudly on the phone about a doctor who had treated him badly. This went on and on until it was finally Michael's turn, he got his x-ray taken, and minutes later the doctor released him with the hardly surprising news that his collar bone was broken. Since a fractured clavicle usually needs to heal by itself, Michael simply received an arm sling which we could have just as well bought at any pharmacy. Further, he got a referral to an orthopedic doctor for follow-up and was offered a pain killer pill, which he declined to take by mouth right away but kept just in case. Weeks later, the first bill came in the mail, followed by a second one a few days later.
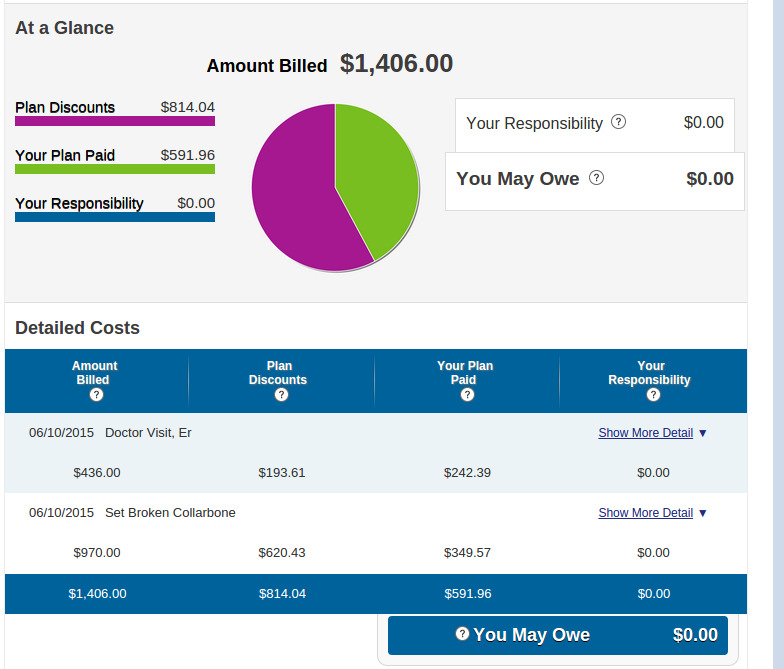
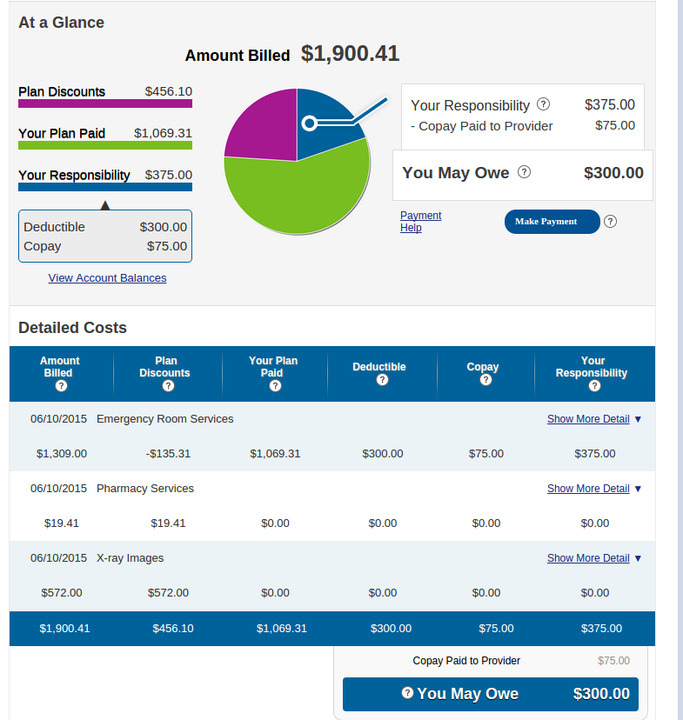
Surprise: For the generic Ibuprofen pill, the ER had charged our health insurance a whopping $19.41, but of course you need to consider that they had an entire team of doctors available ready to squeeze Michael through a CT scanner in an emergency. The total ER bill turned out to $3.306,41, as you can see in Figures 3 and 4. That's the amount that an unsuspecting tourist would have had to pay. But since the ER participates in our health insurer's network, the two parties have agreed on fixed rates for medical procedures, and the health insurance "only" had to pay $1,883.35. We had to chip in $75 as ER co-pay and another $300 deductible which our health plan required. In comparison: For the follow-up visit at the orthopedic specialist, including another set of x-rays, the health insurance only had to pay $177.24, and we forked over $30 in co-pay. You can easily see that it would have been much more cost effective for the health insurance if we had gone to the orthopedic specialist first, but there were no appointments available. In fact, when Michael got the ER's referral, he called the orthopedic doctor's office and the receptionist told him that the next available appointment was in four weeks. When he asked about other doctors in the same office, the receptionist found a less popular one that had an appointment available only a week later.
Stimulated by the ailing state of the American health care system, innovators have come up with capitalist and technical solutions to alleviate the situation. Popular are so-called boutique or concierge doctors. Patients who are willing to sign up for a yearly, monthly, or three-monthly fee can enjoy improved services, like same-day appointments, even on Saturdays, a shorter wait at the doctor's office, and more time with the doctor. Doctors who switch to this model are seeing fewer patients and can focus better on individual cases.

There's many different cost models to choose from. In some, the patient buys the aforementioned conveniences, but claims resulting from visits at doctor's office or lab tests are charged to the patient's health insurance. Another model charges a higher fee, but covers additional services, like seeing a doctor or preventive screenings. Other expenses like immunisations or x-rays are the patient's responsibility. Membership fees range from $150 to $5,000 per year.
The concierge medicine provider "One Medical Group" is currently spreading across San Francisco, with one of their offices being located just around the corner from our house. Critics of this new approach rightfully object that concierge medicine splits patients into first and second class citizens, since not everyone can afford paying the hefty yearly fees. And, what's worse, participating doctors accept fewer patients, exacerbating the effects of the current doctors shortage even further.
Lately, a new trend is making big strides. So-called telemedicine uses video conferences, available today on a wide variety of smart phones and tablets to a broad audience. With the "Doctor on Demand" app downloaded onto their device, patients can enter a video conference with a doctor who is certified to practice in the state the patient resides in. Not having to drive to a doctor's office or wait for days until the next available appointment can be quite advantageous.

Patients simply type in their symptons, along with potential allergies and regularly taken medication, after which they're connected straight with a doctor. Participating doctors are typical primary care physicians handling the usual minor illnesses like the flu, severe head colds, diarrhea, rashes). They're not allowed to treat serious diseases, for these the patient has to visit a doctor's office in person. The video doctors will write prescriptions, though. The fixed price for a virtual session with a doctor is $40. Since this is significantly less expensive than a traditional office visit, one of the major U.S. healthcare providers, United Healthcare, has added the service to their coverage plan.
Even sessions with psychologists are available on "Doctor on Demand". The advantage of this kind of interaction with a doctor is of course that the patient won't have to sit in a waiting room with other sick people, and will get an appointment right away without having to actually drive to the office location. Disadvantages are that the doctor can't examine the patient thoroughly because of the lack of physical contact, and that the personal relationship with the doctor suffers. "Doctor on Demand" is a San Francisco company, by the way. But we're still devoted to our good old primary care physician of 20 years and will dutifully drive to his office whenever we need him.